
A uretero-pelvic junction obstruction is a blockage of urine draining from the kidney at the point where the renal pelvis becomes the ureter. This is a congenital narrowing (present at birth) but can manifest at many ages in life. For many patients, a UPJ obstruction may never need treatment. UPJ obstructions that cause symptoms from blockage of urine flow (pain, infection, kidney stones, loss of kidney function) an excision of the obstructing segment and reconnection of the renal pelvis and ureter corrects the blockage. This surgery is called a Pyeloplasty and is often done robotically.
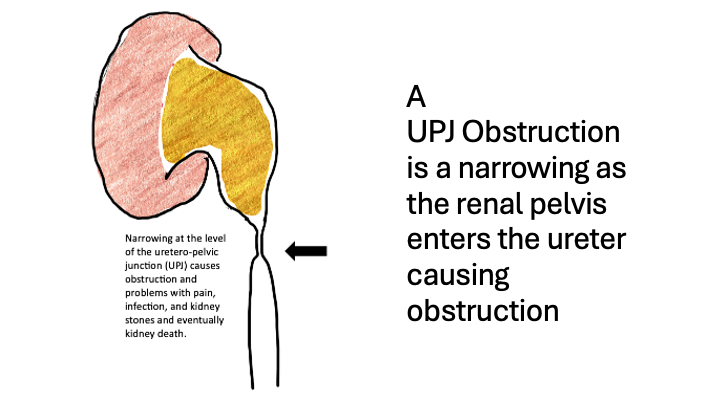
A UPJ (uretero-pelvic junction) obstruction is a condition where urine can’t flow properly from the kidney into the ureter and out of the body. The obstruction point is at the junction between the ureter and the renal pelvis.
Because of the obstruction the renal pelvis dilates, a condition called hydronephrosis. Hydronephrosis can cause symptoms such as pain, kidney stones or risk of infection. Over time a UPJ obstruction that causes high pressures in the kidney can lead to kidney damage.
To understand UPJ obstruction, let’s start with some basics. Each kidney collects urine in a funnel shaped structure called the renal pelvis. From there, the urine is transported by peristalsis to reach the bladder. The connection between the renal pelvis and the ureter is the ureteropelvic junction, or UPJ.”
UPJ obstruction happens when the junction becomes narrowed or blocked. This blockage is most often congenital, meaning present at birth, even if the condition is diagnosed later in life. The obstruction can be acquired later in life due to scarring, kidney stones, injury or surgery.
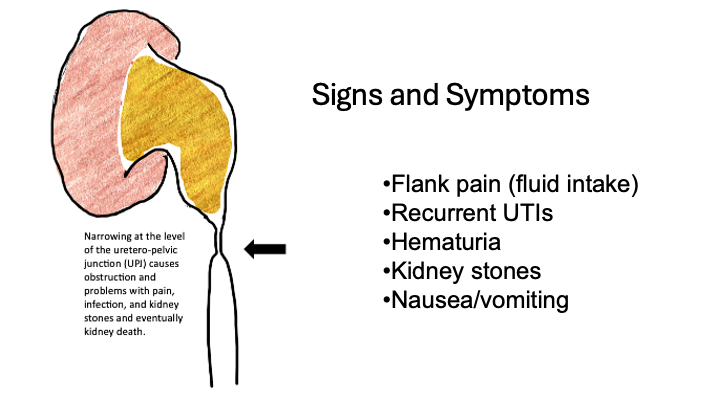
A patient may have an incidental finding of UPJ obstruction but most often they present with symptoms from the obstruction and hydronephrosis. Symptoms vary. Common signs include flank pain—often worse after drinking plenty of fluids—repeated urinary tract infections, kidney stones or a vague sense of abdominal pressure or discomfort.
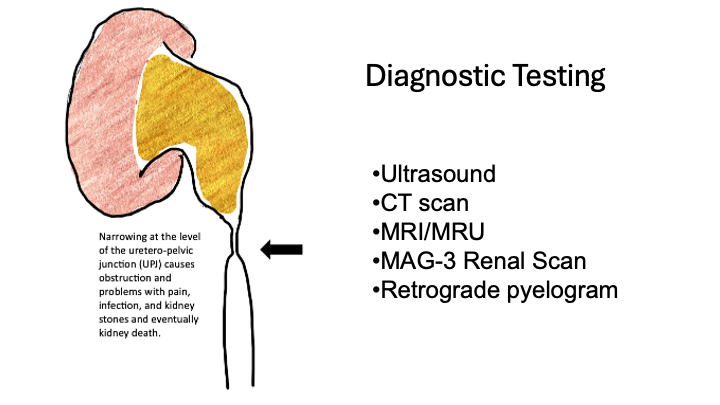
Diagnosis usually starts with a combination of symptom review and clinical history, physical exam, and imaging tests.
An ultrasound can reveal hydronephrosis.
A CT scan helps detect anatomy changes or crossing blood vessels.
MRI urography is especially helpful in children but is not used commonly in adults. Unless a CT is contraindicated that is typically the first choice for imaging.
Ultrasounds, CT and MRI are qualitative studies (ie is there swelling) but do not quantify the level of obstruction.
The test that quantifies the level of obstruction is the nuclear medicine renal scan, which shows how well the urine drains and how much each kidney contributes to total function.”
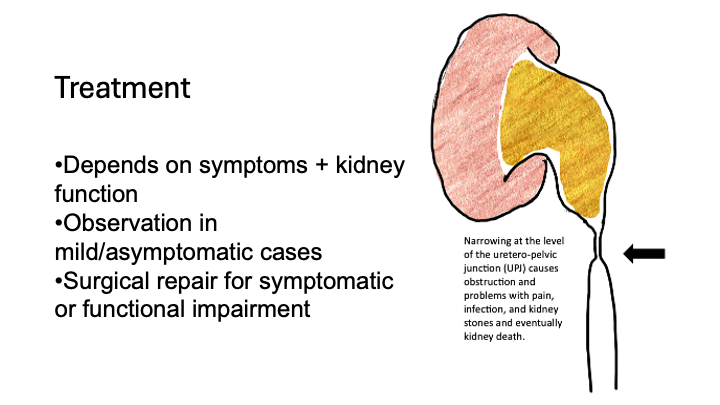
The treatment is surgery. There are no medications for treating UPJ obstruction.
The gold standard treatment is a pyeloplasty. Most often this is done robotically.
The pyeloplasty removes the narrowed section and reconstructs the UPJ to restore normal drainage. Success rates are very high—often above 90%.”
The technique for the procedure is very basic. 1. Identify the point of obstruction/damaged tissue, 2. Remove it, 3. Bring the normal healthier tissue together.
For selected adult patients, an endopyelotomy is a minimally invasive alternative. A small incision is made inside the ureter to widen the junction using a catheter. This does not require entry into the abdomen so there are advantages to the minimally invasive technique. The endopyelotomy has lower success rates than pyeloplasty and is most often not the first choice.
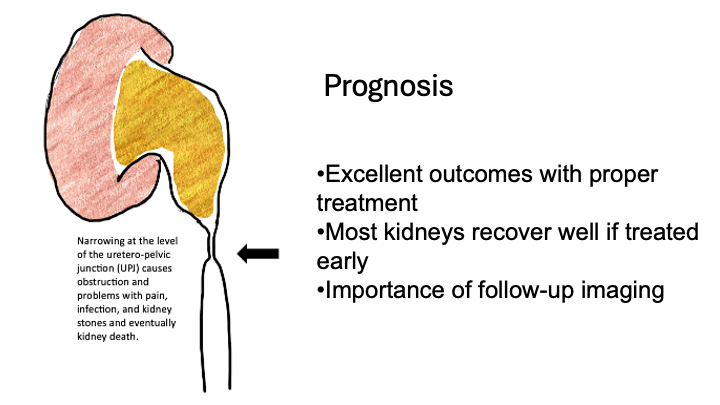
Overall, the prognosis is excellent. The goal is to preserve kidney function and decrease any symptoms from the obstruction. Most people recover kidney function or at least prevent further decline.
Follow-up imaging helps ensure that the repair remains successful.